Medications for GERD Gastroesophageal Reflux Disease (GERD) Treatment
GERD Treatment: Medication
In the event that way of life and dietary changes don't work, your primary care physician might recommend specific meds. There are two classifications of medications for reflux. One reductions the degree of corrosive in your stomach, and one expands the degree of motility (development) in the upper gastrointestinal parcel.
Acid neutralizers
Over-the-counter stomach settling agents are best for irregular and generally rare side effects of reflux. When taken oftentimes, acid neutralizers might demolish the issue. They leave the stomach rapidly, and your stomach really increments corrosive creation therefore.
Receptor blockers
Receptor 2 (H2) blockers are drugs that assist with bringing down corrosive emission. H2 blockers mend esophageal disintegrations in around 50% of patients.
Proton siphon inhibitors
Proton siphon inhibitors (PPIs) are drugs that block the three significant pathways for corrosive creation. PPIs smother corrosive creation considerably more successfully than H2 blockers. PPIs recuperate erosive esophagitis in numerous patients, even those with serious esophageal harm.
Prokinetic specialists
Prokinetic specialists are drugs that improve the movement of the smooth muscle of your gastrointestinal lot. These medications are fairly less powerful than PPIs. Your primary care physician might recommend them in mix with a corrosive stifling medication.
Meds for GERD Gastroesophageal Reflux Disease (GERD) Treatment Video :
Gastroesophageal reflux illness (GERD), gastro-oesophageal reflux illness (GORD), gastric reflux illness, or indigestion illness is characterized as constant side effects or mucosal harm delivered by the unusual reflux of stomach corrosive to the throat.
An ordinary side effect is indigestion. This is normally because of transient or super durable changes in the boundary between the throat and the stomach. This can be because of inadequacy of the lower esophageal sphincter, transient lower esophageal sphincter unwinding, debilitated ejection of gastric reflux from the throat, or a hiatal hernia. An alternate kind of indigestion which produces respiratory and laryngeal indications is laryngopharyngeal reflux (LPR), additionally called extraesophageal reflux infection (EERD). Not at all like GERD, LPR is probably not going to create indigestion, and is accordingly some of the time called quiet reflux.
Heartburn and gastro-oesophageal reflux disease (GORD)
Gastro-oesophageal reflux sickness (GORD) is a typical condition, where corrosive from the stomach spills up into the throat (neck).
It typically happens because of the ring of muscle at the lower part of the throat becoming debilitated. Peruse more about the reasons for GORD.
GORD causes side effects, for example, acid reflux and a terrible desire for the rear of the mouth. It might simply be an incidental disturbance for certain individuals, yet for other people, it very well may be an extreme, deep rooted issue.
GORD can regularly be controlled with self improvement measures and medicine. At times, medical procedure to address the issue might be needed.This theme centers around GORD in grown-ups.
Side effects of GORD can include:
indigestion (an awkward consuming sensation in the chest that frequently happens in the wake of eating)
indigestion (where stomach corrosive returns up into your mouth and causes an undesirable, acrid taste)
oesophagitis (a sore, kindled throat)
awful breath
bulging and burping
feeling or being wiped out
Heartburn and gastro-oesophageal reflux disease (GORD) VIDEO
torment while gulping or potentially trouble gulping
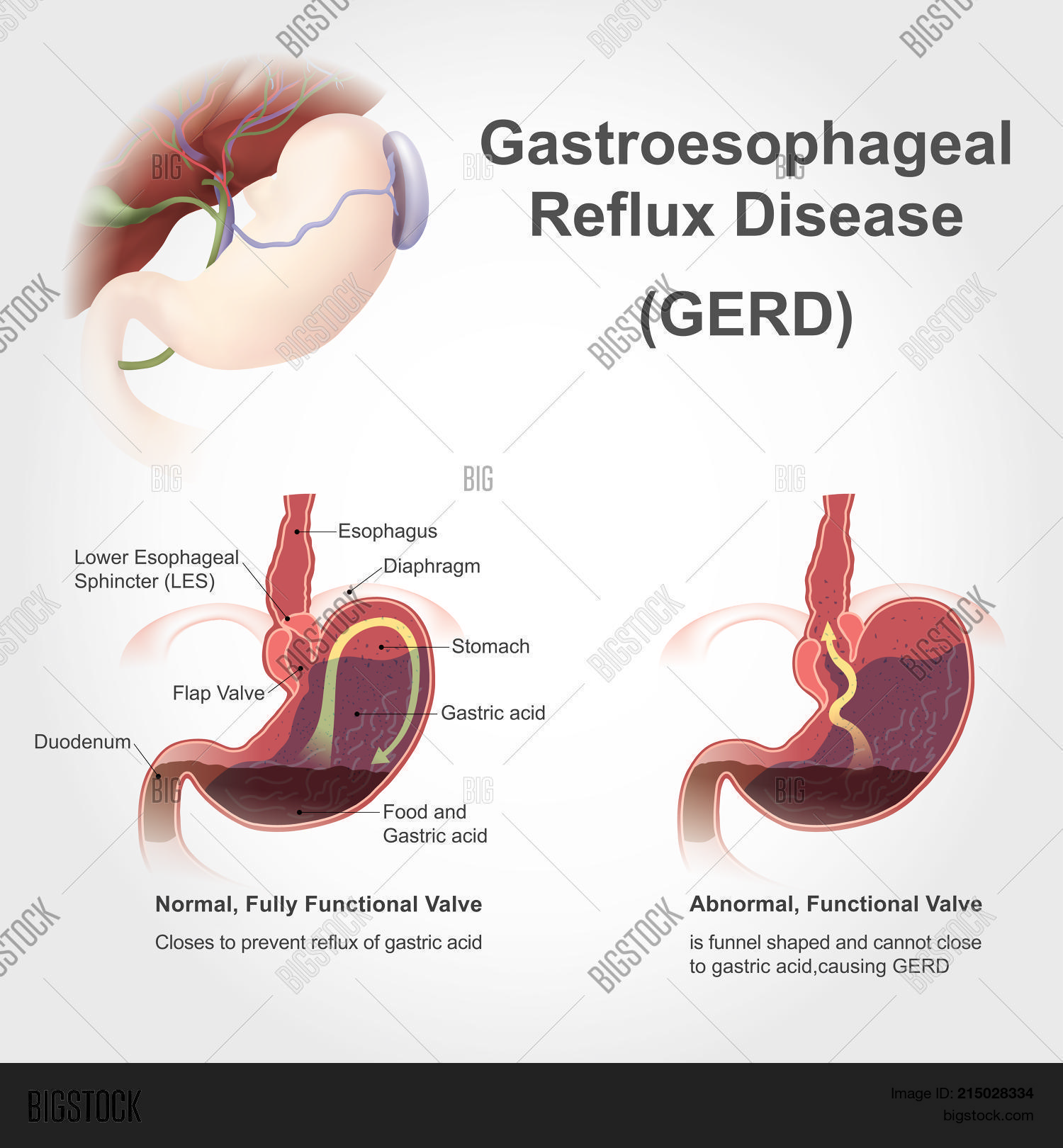
At the entrance to your stomach is a valve, which is a ring of muscle called the lower esophageal sphincter (LES). Normally, the LES closes as soon as food passes through it. If the LES doesn't close all the way or if it opens too often, acid produced by your stomach can move up into your esophagus. This can cause symptoms such as a burning chest pain called heartburn. If acid reflux symptoms happen more than twice a week, you have acid reflux disease, also known as gastroesophageal reflux disease (GERD).
What causes indigestion sickness?
One normal reason for indigestion sickness is a stomach anomaly called a hiatal hernia. This happens when the upper piece of the stomach and LES move over the stomach, a muscle that isolates your stomach from your chest. Regularly, the stomach helps keep corrosive in our stomach. Be that as it may, assuming you have a hiatal hernia, corrosive can climb into your throat and cause side effects of indigestion infection.
These are other normal gamble factors for indigestion sickness:
* Eating huge suppers or resting just after a dinner
* Being overweight or corpulent
* Eating a weighty supper and lying on your back or twisting around at the abdomen
* Nibbling near sleep time
* Eating specific food sources, like citrus, tomato, chocolate, mint, garlic, onions, or zesty or greasy food varieties
* Drinking specific refreshments, like liquor, carbonated beverages, espresso, or tea
* Smoking
* Being pregnant
* Taking headache medicine, ibuprofen, certain muscle relaxers, or circulatory strain prescriptions
Gastroesophageal / Acid Reflux Disease At A Glance
* Gastroesophageal/Acid Reflux Disease is a condition where the fermented fluid substance of the stomach upholds into the throat.
* The reasons for GERD incorporate an unusual lower esophageal sphincter, hiatal hernia, strange esophageal constrictions, and slow exhausting of the stomach.
* Gastroesophageal/Acid Reflux Disease might harm the covering of the throat, along these lines causing aggravation (esophagitis), albeit typically it doesn't.
* The side effects of straightforward GERD are indigestion, spewing forth, and sickness.
* Difficulties of GERD incorporate ulcers and injuries of the throat, Barrett's throat, hack and asthma, throat and laryngeal irritation, aggravation and contamination of the lungs, and assortment of liquid in the sinuses and center ear.
* Barrett's throat is a pre-destructive condition that requires occasional endoscopic observation for the advancement of malignant growth.
* Gastroesophageal/Acid Reflux Disease might be analyzed or assessed by a preliminary of treatment, endoscopy, biopsy, x-beam, assessment of the throat and larynx, 24 hour esophageal corrosive testing, esophageal motility testing, exhausting investigations of the stomach, and esophageal corrosive perfusion.
* GERD is treated with way of life changes, acid neutralizers, receptor bad guys (H2 blockers), proton siphon inhibitors (PPIs), favorable to motility drugs, froth boundaries, medical procedure, and endoscopy.
Gastroesophageal / Acid Reflux Disease At A Glance VIDEO
What is a reasonable approach to the management of Gastroesophageal / Acid Reflux Disease?
There are several ways to approach the evaluation and management of Gastroesophageal / Acid Reflux Disease. The approach depends primarily on the frequency and severity of symptoms, the adequacy of the response to treatment, and the presence of complications.
For infrequent heartburn, the most common symptom of Gastroesophageal / Acid Reflux Disease, life-style changes and an occasional antacid may be all that is necessary. If heartburn is frequent, daily non-prescription-strength (over-the-counter) H2 antagonists may be necessary. A foam barrier also can be used with the antacid or H2 antagonist.
If life-style changes and antacids, non-prescription H2 antagonists, and a foam barrier do not adequately relieve heartburn, it is time to see a physician for further evaluation and to consider prescription-strength drugs. The evaluation by the physician should include an assessment for possible complications of GERD based on the presence of such symptoms or findings as:
* cough,
* asthma,
* hoarseness,
* sore throat,
* difficulty swallowing,
* unexplained lung infections, or
* anemia (due to bleeding from esophageal inflammation or ulceration).
Clues to the presence of diseases that may mimic Gastroesophageal / Acid Reflux Disease, such as gastric or duodenal ulcers and esophageal motility disorders, should be sought.
If there are no symptoms or signs of complications and no suspicion of other diseases, a therapeutic trial of acid suppression with H2 antagonists often is used. If H2 antagonists are not adequately effective, a second trial, with the more potent PPIs, can be given. Sometimes, a trial of treatment begins with a PPI and skips the H2 antagonist. If treatment relieves the symptoms completely, no further evaluation may be necessary and the effective drug, the H2 antagonist or PPI, is continued. As discussed previously, however, there are potential problems with this commonly used approach, and some physicians would recommend a further evaluation for almost all patients they see.
If at the time of evaluation, there are symptoms or signs that suggest complicated Gastroesophageal / Acid Reflux Disease or a disease other than GERD or if the relief of symptoms with H2 antagonists or PPIs is not satisfactory, a further evaluation by endoscopy (EGD) definitely should be done.
There are several possible results of endoscopy and each requires a different approach to treatment. If the esophagus is normal and no other diseases are found, the goal of treatment simply is to relieve symptoms. Therefore, prescription strength H2 antagonists or PPIs are appropriate. If damage to the esophagus (esophagitis or ulceration) is found, the goal of treatment is healing the damage. In this case, PPIs are preferred over H2 antagonists because they are more effective for healing.
If complications of Gastroesophageal / Acid Reflux Disease, such as stricture or Barrett's esophagus are found, treatment with PPIs also is more appropriate. However, the adequacy of the PPI treatment probably should be evaluated with a 24-hour pH study during treatment with the PPI. (With PPIs, although the amount of acid reflux may be reduced enough to control symptoms, it may still be abnormally high. Therefore, judging the adequacy of suppression of acid reflux by only the response of symptoms to treatment is not satisfactory.) Strictures may also need to be treated by endoscopic dilatation (widening) of the esophageal narrowing. With Barrett's esophagus, periodic endoscopic examination should be done to identify pre-malignant changes in the esophagus.
If symptoms of GERD do not respond to maximum doses of PPI, there are two options for management. The first is to perform 24-hour pH testing to determine whether the PPI is ineffective or if a disease other than Gastroesophageal / Acid Reflux Disease is likely to be present. If the PPI is ineffective, a higher dose of PPI may be tried. The second option is to go ahead without 24 hour pH testing and to increase the dose of PPI. Another alternative is to add another drug to the PPI that works in a way that is different from the PPI, for example, a pro-motility drug or a foam barrier. If necessary, all three types of drugs can be used. If there is not a satisfactory response to this maximal treatment, 24 hour pH testing should be done.
Who should consider surgery or, perhaps, an endoscopic treatment trial for GERD? (As mentioned previously, the effectiveness of the recently developed endoscopic treatments remains to be determined.) Patients should consider surgery if they have regurgitation that cannot be controlled with drugs. This recommendation is particularly important if the regurgitation results in infections in the lungs or occurs at night when aspiration into the lungs is more likely. Patients also should consider surgery if they require large doses of PPI or multiple drugs to control their reflux. Still, it is debated whether or not a desire to be free of the need to take life-long drugs to prevent symptoms of Gastroesophageal / Acid Reflux Disease is by itself a satisfactory reason for having surgery.
What is a reasonable approach to the management of Gastroesophageal / Acid Reflux Disease? VIDEO
How is Gastroesophageal / Acid Reflux Disease treated?
Life-style changes
One of the simplest treatments for Gastroesophageal / Acid Reflux Disease is referred to as life-style changes, a combination of several changes in habit, particularly related to eating.
As discussed above, reflux of acid is more injurious at night than during the day. At night, when individuals are lying down, it is easier for reflux to occur. The reason that it is easier is because gravity is not opposing the reflux, as it does in the upright position during the day. In addition, the lack of an effect of gravity allows the refluxed liquid to travel further up the esophagus and remain in the esophagus longer. These problems can be overcome partially by elevating the upper body in bed. The elevation is accomplished either by putting blocks under the bed's feet at the head of the bed or, more conveniently, by sleeping with the upper body on a wedge.
These maneuvers raise the esophagus above the stomach and partially restore the effects of gravity. It is important that the upper body and not just the head be elevated. Elevating only the head does not raise the esophagus and fails to restore the effects of gravity.
Elevation of the upper body at night generally is recommended for all patients with Gastroesophageal / Acid Reflux Disease. Nevertheless, most patients with GERD have reflux only during the day and elevation at night is of little benefit for them. It is not possible to know for certain which patients will benefit from elevation at night unless acid testing clearly demonstrates night reflux. However, patients who have heartburn, regurgitation, or other symptoms of GERD at night are probably experiencing reflux at night and definitely should use upper body elevation. Reflux also occurs less frequently when patients lie on their left rather than their right sides.
Gastroesophageal / Acid Reflux DiseaseDiet
Several changes in eating habits can be beneficial in treating GERD. Reflux is worse following meals. This probably is so because the stomach is distended with food at that time and transient relaxations of the lower esophageal sphincter are more frequent. Therefore, smaller and earlier evening meals may reduce the amount of reflux for two reasons. First, the smaller meal results in lesser distention of the stomach. Second, by bedtime, a smaller and earlier meal is more likely to have emptied from the stomach than is a larger one. As a result, reflux is less likely to occur when patients with Gastroesophageal / Acid Reflux Disease lie down.
Certain foods are known to reduce the pressure in the lower esophageal sphincter and thereby promote reflux. These foods should be avoided and include:
* chocolate,
* peppermint,
* alcohol, and
* caffeinated drinks.
Fatty foods (which should be decreased) and smoking (which should be stopped) also reduce the pressure in the sphincter and promote reflux.
In addition, patients with Gastroesophageal / Acid Reflux Disease may find that other foods aggravate their symptoms. Examples are spicy or acid-containing foods, like citrus juices, carbonated beverages, and tomato juice. These foods should also be avoided.
One novel approach to the treatment of Gastroesophageal / Acid Reflux Disease is chewing gum. Chewing gum stimulates the production of more bicarbonate-containing saliva and increases the rate of swallowing. After the saliva is swallowed, it neutralizes acid in the esophagus. In effect, chewing gum exaggerates one of the normal processes that neutralizes acid in the esophagus. It is not clear, however, how effective chewing gum actually is in treating heartburn. Nevertheless, chewing gum after meals is certainly worth a try.
How is Gastroesophageal / Acid Reflux Disease treated? VIDEO
What are the complications of Gastroesophageal / Acid Reflux Disease?
Ulcers
The fluid from the stomach that refluxes into the throat harms the cells coating the throat. The body answers in the manner that it for the most part answers harm, which is with aggravation (esophagitis). The motivation behind aggravation is to kill the harming specialist and start the method involved with recuperating. Assuming the harm goes profoundly into the throat, a ulcer structures. A ulcer is basically a break in the covering of the throat that happens in a space of aggravation.
Ulcers and the extra aggravation they incite may disintegrate into the esophageal veins and bring about seeping into the throat. Sporadically, the draining is extreme and may require:
* blood bondings,
* an endoscopic technique (wherein a cylinder is embedded through the mouth into the throat to envision the site of draining and to stop the dying), or
* careful treatment. Injuries Ulcers of the throat mend with the development of scars (fibrosis)
Over the long run, the scar tissue psychologists and river the lumen (inward cavity) of the throat. This scarred restricting is known as an injury. Gulped food might stall out in the throat once the limiting becomes sufficiently extreme (normally when it confines the esophageal lumen to a distance across of one centimeter). The present circumstance might require endoscopic evacuation of the stuck food. Then, to keep food from staying, the limiting should be extended (enlarged). Additionally, to forestall a repeat of the injury, reflux likewise should be forestalled.
Barrett's throat
Well established or potentially extreme Gastroesophageal/Acid Reflux Disease causes changes in the cells that line the throat in certain patients. These cells are pre-dangerous lastly become destructive. This condition is alluded to as Barrett's throat and happens in around 10% of patients with GERD. The kind of esophageal disease related with Barrett's throat (adenocarcinoma) is expanding in recurrence. It isn't clear why a few patients with Gastroesophageal/Acid Reflux Disease foster Barrett's throat, however most don't. Barrett's throat can be perceived outwardly at the hour of an endoscopy and affirmed by minute assessment of biopsies of the coating cells.
Then, at that point, patients with Barrett's throat might require intermittent observation endoscopies with biopsies. The motivation behind reconnaissance is to identify pre-harmful changes with the goal that disease forestalling treatment can be begun. It is additionally accepted that patients with Barrett's throat ought to get most extreme treatment for Gastroesophageal/Acid Reflux Disease to forestall further harm to the throat. Systems are being concentrated on that eliminate the strange covering cells. A few endoscopic, non-careful methods can be utilized to eliminate the cells. These procedures are alluring on the grounds that they don't need a medical procedure; nonetheless, there are related complexities, and the drawn out viability of the therapies has not entirely set in stone. Careful expulsion of the throat is generally a choice. For additional, kindly perused the Barrett's Esophagus article.
Hack and asthma
Many nerves are in the lower throat. A portion of these nerves are animated by the refluxed corrosive, and this feeling brings about torment (typically indigestion). Different nerves that are animated don't deliver torment. All things considered, they invigorate yet different nerves that incite hacking. Along these lines, refluxed fluid can cause hacking while never arriving at the throat! Along these lines, reflux into the lower throat can invigorate esophageal nerves that interface with and can animate nerves going to the lungs.
These nerves to the lungs then, at that point, can make the more modest breathing cylinders limited, bringing about an assault of asthma. Gastroesophageal/Acid Reflux Disease is a typical reason for unexplained hacking. Despite the fact that GERD likewise might be a reason for asthma, almost certainly, it encourages asthmatic assaults in patients who as of now have asthma. Albeit persistent hack and asthma are normal sicknesses, it isn't clear exactly how frequently they are bothered or brought about by GERD. Irritation of the throat and larynx If refluxed fluid moves beyond the upper esophageal sphincter, it can enter the throat (pharynx) and, surprisingly, the voice box (larynx). The subsequent aggravation can prompt an irritated throat and raspiness.
Likewise with hacking and asthma, it isn't clear exactly how normally GERD is liable for in any case unexplained irritation of the throat and larynx. Aggravation and disease of the lungs Refluxed fluid that passes the larynx can enter the lungs. The reflux of fluid into the lungs (called goal) frequently brings about hacking and gagging. Goal, be that as it may, can likewise happen without delivering these side effects. Regardless of these side effects, yearning might prompt disease of the lungs and result in pneumonia. This sort of pneumonia is a not kidding issue requiring prompt treatment. Whenever goal is unaccompanied by side effects, it can bring about a sluggish, moderate scarring of the lungs (aspiratory fibrosis) that should be visible on chest x-beams. Yearning is bound to happen around evening time since that is the point at which the cycles (components) that safeguard against reflux are not dynamic and the hacking reflex that safeguards the lungs additionally isn't dynamic.
Liquid in the sinuses and center ears
The throat speaks with the nasal sections. In little youngsters, two patches of lymph tissue, called the adenoids, are found where the upper piece of the throat joins the nasal sections. The sections from the sinuses and the cylinders from the center ears (Eustachian tubes) open into the back of the nasal entries close to the adenoids. Refluxed fluid that enters the upper throat can aggravate the adenoids and influence them to enlarge. The enlarged adenoids then, at that point, can impede the entries from the sinuses and the Eustachian tubes. When the sinuses and center ears are shut off from the nasal entries by the expanding of the adenoids, liquid collects inside them. This collection of liquid can prompt inconvenience in the sinuses and ears. Since the adenoids are noticeable in little youngsters, and not in grown-ups, this liquid collection in the ears and sinuses is found in kids and not grown-ups.
Indigestion Disease
What are the complications of Gastroesophageal / Acid Reflux Disease? VIDEO
Who Needs Gastroesophageal / Acid Reflux Disease Treatment?
There are many valid justifications to treat Gastroesophageal/Acid Reflux Disease. In the first place, GERD treatment encourages you. Living with uncontrolled GERD - - the aggravation, the hack, the restless evenings - - can be extreme. "Gastroesophageal/Acid Reflux Disease puts truly a weight on an individual's personal satisfaction," says Goutham Rao, MD. Rao is a board individual from the National Heartburn Alliance and an academic partner at the University of Pittsburgh School of Medicine. "GERD," he says, "can be really crippling." Second, GERD/Acid Reflux Disease represents some genuine long haul wellbeing gambles. Over the long haul, the harm to the throat can cause difficulties. One of those is a condition called Barrett's throat, which is related with a little however critical gamble of esophageal disease. Luckily, GERD/Acid Reflux Disease treatment can keep Barrett's throat from creating. How can you say whether you really want treatment for Gastroesophageal/Acid Reflux Disease? What's the distinction between innocuous acid reflux and more genuine GERD? It's not such a lot of the seriousness, specialists say, yet the recurrence. The standard proposal is that anybody with side effects at least two times each week ought to see a specialist. Cheskin is more mindful. He says that even side effects that happen just once seven days ought to be looked at. "Throughout the long term," he says, "even that degree of acid reflux can cause harm." Sometimes the clearest difficult situation is the means by which regularly you use over-the-counter (OTC) medicines for indigestion help. Heartburn Disease
Now is the ideal time to see your PCP assuming you have indigestion side effects at least two times each week or then again on the off chance that drugs don't bring enduring help. Side effects, for example, indigestion are the way in to the conclusion of heartburn sickness, particularly on the off chance that way of life changes, stomach settling agents, or corrosive hindering meds assist with decreasing these side effects. In the event that these means don't help or then again assuming you have successive or extreme indigestion infection side effects, your PCP might arrange tests to affirm an analysis and check for different issues.
You might require at least one tests, for example, these:
* Barium swallow (esophagram) can check for ulcers or a restricting of the throat. You first swallow an answer for assist structures with appearing on a X-beam.
* Esophageal manometry can actually take a look at the capacity of the throat and lower esophageal sphincter.
* pH observing can check for corrosive in your throat. The specialist embeds a gadget into your throat and passes on it set up for one to two days to gauge how much corrosive in your throat.
* Endoscopy can check for issues in your throat or stomach. This test includes embedding a long, adaptable, lit tube down your throat. In the first place, the specialist will splash the rear of your throat with sedative and give you a narcotic to make you more agreeable.
* A biopsy might be takenduring endoscopy to actually take a look at tests of tissue under a magnifying instrument for disease or irregularities
What are the symptoms of uncomplicated Gastroesophageal Reflux Disease ?
The side effects of simple Gastroesophageal Reflux Disease are principally indigestion, spewing forth, and sickness. Different side effects happen when there are entanglements of GERD and will be examined with the confusions. Indigestion When heartburns back into the throat in patients with Gastroesophageal/Acid Reflux Disease, nerve strands in the throat are animated. This nerve feeling results most ordinarily in indigestion, the aggravation that is normal for GERD/Acid Reflux Disease. Acid reflux typically is depicted as a consuming aggravation in the chest. It might begin high in the mid-region or may stretch out up into the neck. In certain patients, nonetheless, the torment might be sharp or tension like, as opposed to consuming. Such agony can impersonate heart torment (angina). In different patients, the aggravation might reach out to the back. Since indigestion is more normal after suppers, acid reflux is more normal after dinners. Indigestion is likewise more normal when people rests on the grounds that without the impacts of gravity, reflux happens all the more effectively, and corrosive is gotten back to the stomach all the more leisurely.
Numerous patients with Gastroesophageal/Acid Reflux Disease are stirred from rest by indigestion. Episodes of indigestion might happen rarely or much of the time, yet episodes will more often than not occur occasionally. This implies that the episodes are more incessant or serious for a time of a little while or months, and afterward they become less continuous or extreme or even missing for quite some time or months. This periodicity of side effects gives the reasoning to irregular treatment in patients with Gastroesophageal/Acid Reflux Disease who don't have esophagitis. By the by, indigestion is a long lasting issue, and it quite often returns. Disgorging Regurgitation is the presence of refluxed fluid in the mouth. In many patients with GERD, generally just little amounts of fluid arrive at the throat, and the fluid remaining parts in the lower throat. Periodically in certain patients with GERD, bigger amounts of fluid, now and then containing food, are refluxed and arrive at the upper throat. At the upper finish of the throat is the upper esophageal sphincter (UES). The UES is a roundabout ring of muscle that is practically the same in its activities to the LES.
That is, the UES keeps esophageal substance from upholding into the throat. Whenever modest quantities of refluxed fluid and additionally food sources break (overcome) the UES and enter the throat, there might be a corrosive desire for the mouth. Assuming bigger amounts break the UES, patients may unexpectedly observe their mouths loaded up with the fluid or food. Likewise, regular or delayed disgorging can prompt corrosive instigated disintegrations of the teeth. Queasiness Nausea is extraordinary in Gastroesophageal/Acid Reflux Disease. In certain patients, notwithstanding, it very well might be continuous or extreme and may bring about heaving. As a matter of fact, in patients with unexplained queasiness and additionally spewing, GERD is one of the principal conditions to be thought of. It isn't clear why a few patients with GERD grow predominantly indigestion and others grow basically queasiness.